CHMP Meeting Highlights August 2021
The written procedure of CHMP in August does not include the relevant decisions we would report in CRISP. However, we use this welcome break to highlight the 10th anniversary of the European marketing authorization for ipilimumab. This authorisation of the first checkpoint inhibitor marks 10 years of unprecedented success for immunotherapy of cancer, and was the beginning of a success story continuing until today.
Ten years marketing authorization ipilimumab, ten years of successful cancer immunotherapy
First successful cancer immunotherapies (1998-2005)
For decades, basic research and clinical trials aimed for the establishment of a meaningful cancer immunotherapy. Repeatedly, promising approaches had ultimately failed to deliver the outstanding clinical benefit everyone had hoped for. Ten years ago, in 2011, and despite high hopes, it seemed that, once again, we would not see true game changers and a subsequent plethora of licensed medicines.
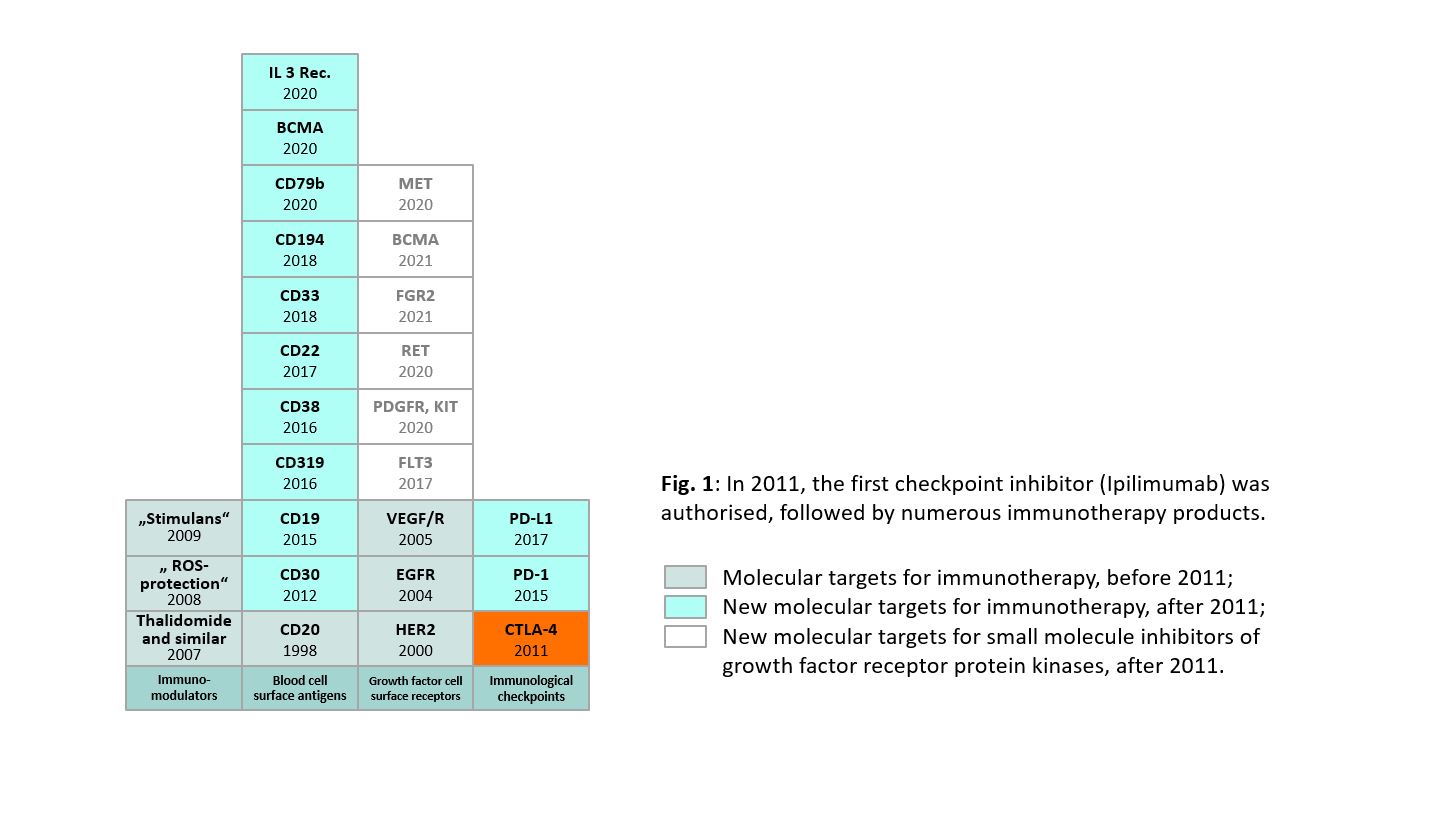
Monoclonal antibodies (mAbs) had long arrived at cancer therapy. In 1998, rituximab was approved for the “treatment of patients with stage III-IV follicular lymphoma who are chemoresistant or are in their second or subsequent relapse after chemotherapy”. This established that targeting blood cell surface antigens with mAbs was a clinically valid concept for the treatment of haematological neoplasms. Two years later, in 2000, trastuzumab, targeting HER2 on the breast cancer cells, established that targeting cell surface antigens with mAb was a clinically valid concept for the treatment of solid tumours.
This was further substantiated when cetuximab, targeting the EGF receptor, was approved for the treatment of colorectal cancer in 2004. In 2005, bevacizumab was approved, the first product that successfully used the VEGF-VEGF receptor signalling pathway as pharmacological target (Figure 1). Regardless of high hopes that many more mAbs for the therapy of cancer would soon follow on these pioneering products, this did not happen for several years.
The years between 2005 and 2011 remained without any other growth factor or growth factor receptor as target for monoclonal antibody in cancer therapy; and no further blood cell surface antigens could be established as additional targets for haematological neoplasms during this time.
{kind=link}
Immune-modulators for cancer therapy (2005-2011)
For several years, no mAbs against another target received a marketing authorization for the treatment of cancer. In this lag-phase of anti-cancer mAbs, from 2005 to 2011, a mixed group of “immune-modulators” tried to fill the gap. The most important innovation was the use of the thalidomide class (2007) for the treatment of multiple myeloma (MM) and related neoplasia. While it is generally accepted that a stimulation of the immune response contributes to their efficacy against MM, our understanding of the exact pharmacological mechanism(s) or mode of action of thalidomide, lenalidomide and pomalidomide has still remains elusive. Moreover, thalidomide was never developed as an immunotherapy in the first place. The discovery of thalidomide’s effectiveness against MM is a serendipity rather than a success of strategically planned research.
The development of thalidomide and its analogues into approvable products is a good example for the value of repurposing, even including repurposing-specific challenges such as concerns of victims of the previous use of a substance. For thalidomide and related products, it was important to include both the concerns of victims of the previous use and the hopes of MM patients for its future use. During the assessment of the marketing authorization application of lenalidomide (the first approved thalidomide analogue), the European Medicines Agency invited thalidomide victims and myeloma patients to discuss benefits and risks including ethical concerns and the content of the risk management plan, package leaflet and labelling.
In 2008, histamine was granted a European marketing authorization for the treatment of acute myeloid leukaemia (AML) in combination with interleukin-2. It has not been widely used, has not been approved by FDA, and its pharmacological mechanism is not completely understood but presumed to be the protection of immune cells by inhibiting the formation of reactive oxygen species.
In 2009, mifamurtide was authorised for the treatment of osteosarcoma. As immunomodulator, mifamurtide stimulates monocytes and macrophages. Regardless of this seemingly basic stimulation of the immune system, mifamurtide remained a niche product for the treatment of sarcoma.
Overall, none of these products seemed to exert a pharmacological mechanism or use a molecular target that would allow the broad expansion to other tumour types.
Widespread use of mAbs for the immune-therapy of cancer (2011- )
The authorisation of ipilimumab in 2011 was the beginning of 10 very successful years for mAbs and the immunotherapy of cancer and several new targets have been identified and successfully used. There are three major groups of targets for mAbs used in immune oncology: blood cell surface antigens, growth factor signalling and immunologic checkpoints.
Targeting blood cell surface antigens
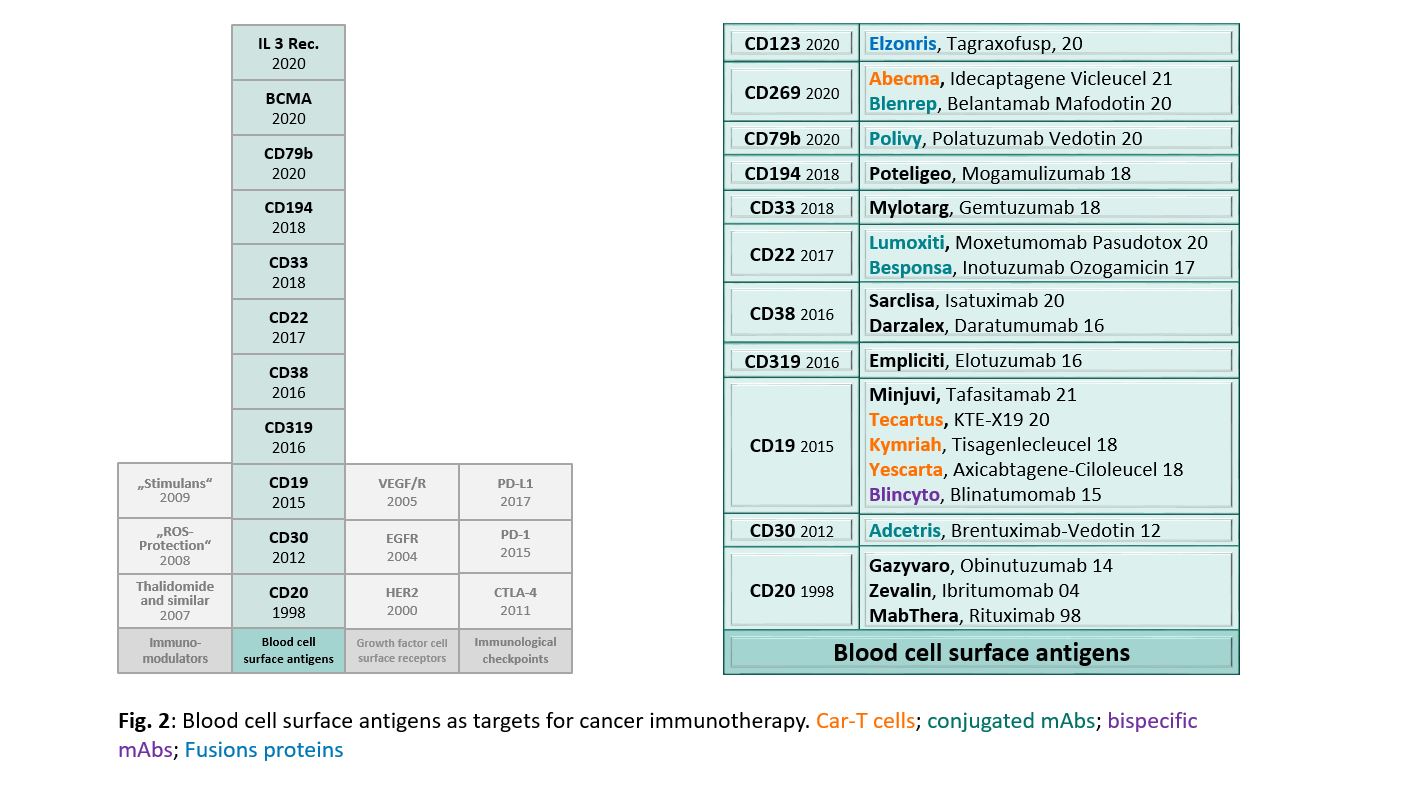
Since 2011, several mAbs against blood cell surface antigens have been approved for the treatment of hematologic neoplasia (Figure 2). Almost all targeted antigens are characteristic for the B cell lineage, with the exception of CD194, which is expressed on T-cells, and CD123, which is expressed on pluripotent progenitor cells, basophilic granulocytes and dendritic cells. In addition to “normal” mAbs, antibody-drug conjugates against CD22 (inotuzumab ozogamicin and moxetumomab pasudotox), CD79b (polatuzumab vedotin), and CD269 (belantamab mafodotin) have been developed.
The latter being also targeted by CAR-T cells (idecaptagene vicleucel). CD19 is used as a target not only for a “normal” mAb (tafasitamab), but as well for the bispecific blinatumomab and for the three CAR-T cells axicabtagene-ciloleucel, tisagenlecleucel and KTE-X19.
{kind=link}
Targeting growth factors and growth factor receptors
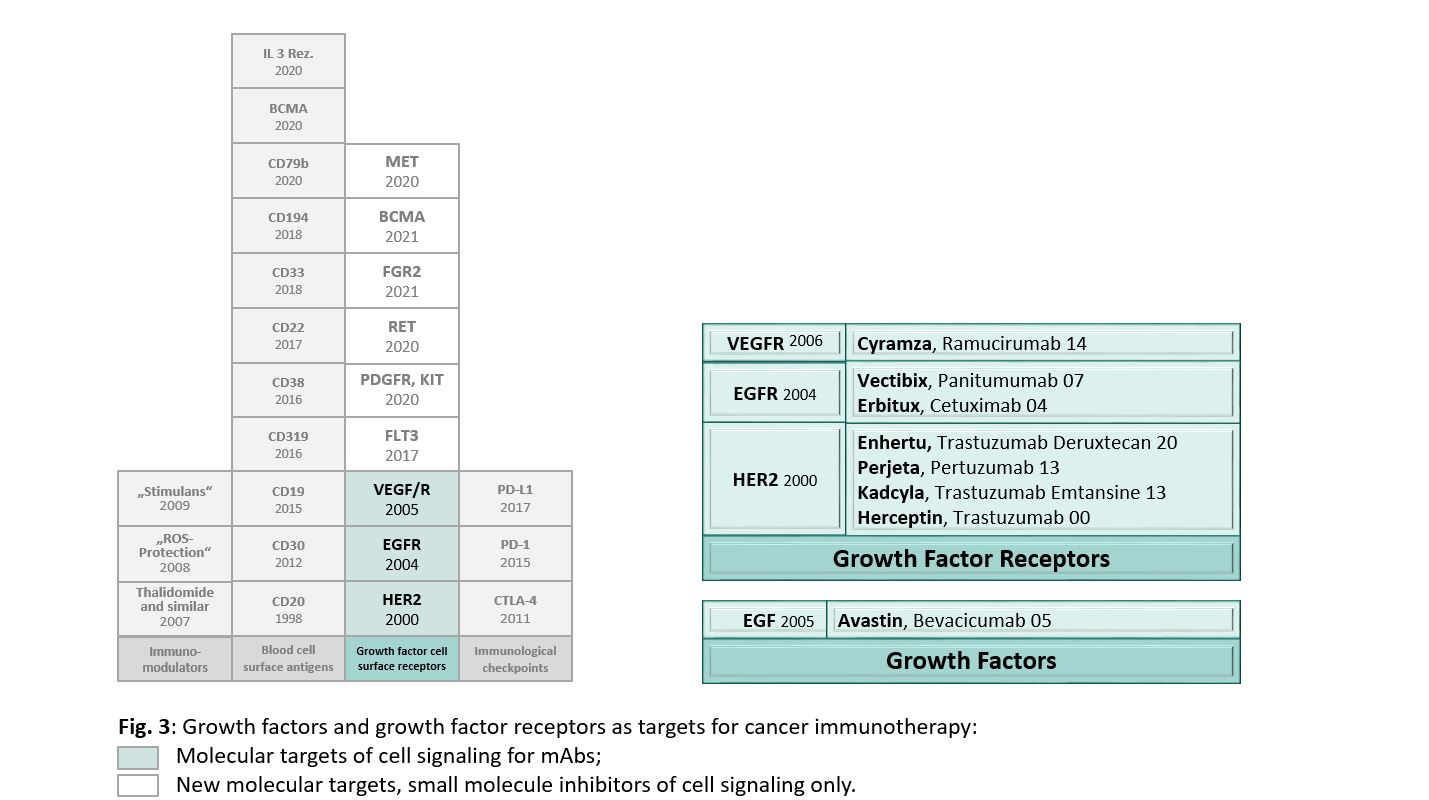
In 2000, the marketing authorisation for trastuzumab showed that mAbs against growth factor receptors on solid tumours can have an outstanding efficacy. When cetuximab, targeting EGFR, was approved in 2004, the validity of this approach was confirmed. Building on the success of trastuzumab, more HER2 mAbs, including conjugated antibodies, have been introduced. Similarly, additional mAbs against EGFR followed on cetuximab (Figure 3). At variance with cetuximab, the indication of panitumumab, although similar to cetuximab targeting EGFR, is not restricted to EGFR-expressing tumours. Another anti-EGFR mAb, necitumumab, which similar to cetuximab was indicated only for tumours expressing EGFR, is no longer available in the EU. The marketing authorisation holder (Eli Lilly) of necitumumab (® Portrazza) did not apply for the renewal of the marketing authorisation as there was not sufficient demand for the product in the EU.
In the following years, more growth factor receptors where successfully used for the development of therapies for solid tumours (although more frequently with small molecule protein kinase inhibitors than with mAbs). Signalling by VEGF / VEGFR was first used as the pharmacological principle of bevacicumab (anti VEGF) authorised in 2005. Later, in 2014, ramucirumab targeting not VEGF but the VEGF receptor was authorized, albeit not the first to target VEGFR. Preceding ramucirumab, several small molecules inhibiting VEGF receptor’s tyrosine kinase had been approved. Currently, the development of new therapeutic approaches using growth factor receptors as targets is mostly driven by small molecule protein kinase inhibitors. The receptors targeted by these new classes of protein kinase inhibitors are shown in Figure 3.
{kind=link}
Targeting immunologic checkpoints
The most dynamic development of cancer immunotherapy has been in the group of checkpoint inhibitors. While ipilimumab has the honour of being the first checkpoint inhibitor ever approved for the treatment of cancer and ushered in the new era, it has a much narrower use than its successors. Unless in combination with another checkpoint inhibitor, on its own it is effective only against melanoma.
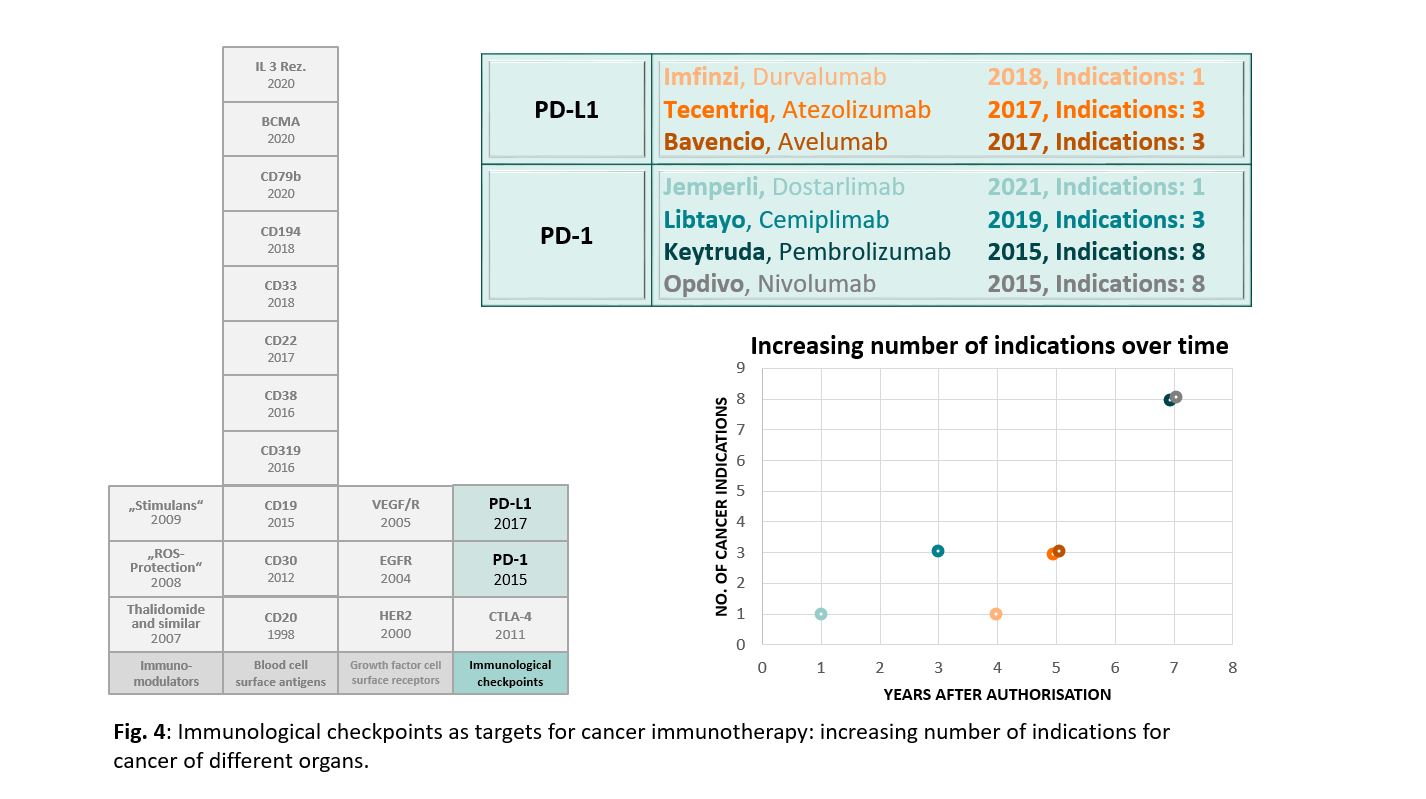
Today’s flagship of cancer immunotherapy is the inhibition of the interaction of PD-1 and PD-L1. The mere number of mAbs targeting PD-1/PD-L1 illustrates the dynamic in this field. Currently, in August 2021, seven mAbs have been approved and more are underway (Figure 4). No other molecular target in oncology has attracted that many mAbs in such a short time. Only antibodies against CD20 come close, with three approved products. These, however, accumulated over a time span of 16 years after rituximab was first approved in 1998.
That dynamic development of these checkpoint inhibitors in cancer immunotherapy is further evidenced by an increasingly broad use of the same products against more and more different cancer types. While effectiveness against several tumour types is common for the time-tested cytotoxic and genotoxic anti-cancer treatments, mAbs for the treatment of cancer have usually less indications. Not only are the mAbs against blood cell surface antigens limited to haematological indications, mAbs against growth factor receptors such as EGFR or HER2 usually target cancer of only one or two organs, with the exception of mAbs against VEGF and VEGFR, bevacizumab (six organs) and ramucirumab (four organs). At variance, both nivolumab and pembrolizumab each target cancer of seven different organs.
{kind=link}
Previous CHMP Meeting Highlights can be accessed at: https://www.basg.gv.at/en/healthcare-professionals/chmp-meeting-highlights-basg